
MAP scientist Dr. Tara Gomes is quoted in Toronto Star about health concerns related to the drug poisoning crisis. Hayley Thompson, project manager of Toronto Drug Checking Service, is also mentioned, reporting that the average amount of medetomidine (an animal tranquilize) found in fentanyl samples has increased in the past year.
Author: Samira Prasad
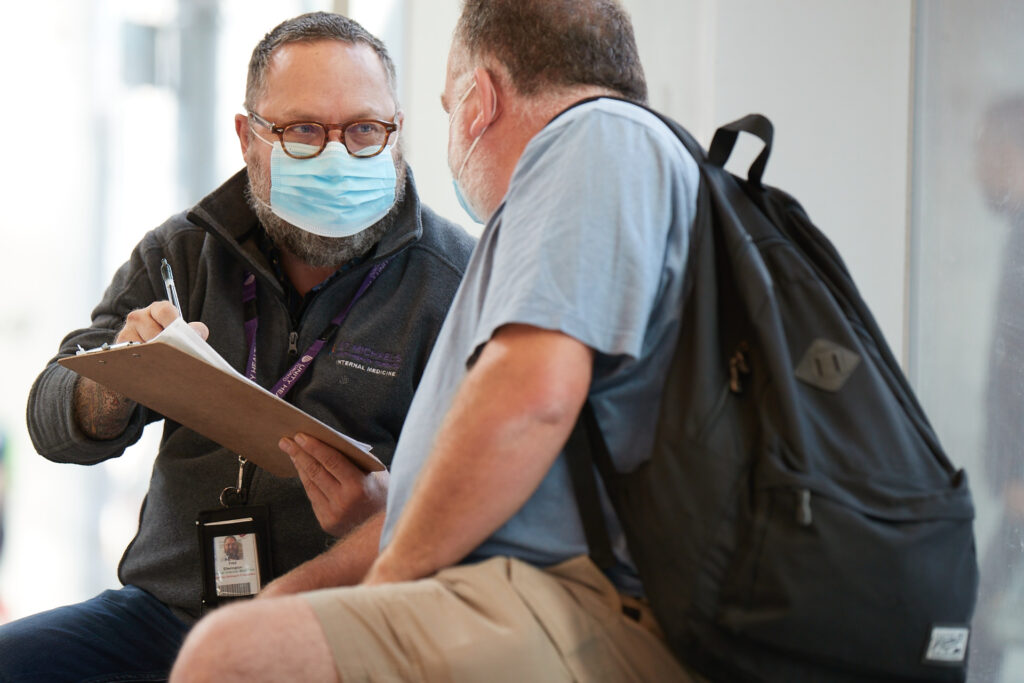
New research affirms construction workers disproportionately affected by opioid deaths

A new study lead by MAP scientist Dr. Tara Gomes, found that construction and trades workers accounted for approximately one-third of opioid toxicity deaths in Ontario where occupation was known between 2018 and 2024.
“I think a lot of people have a picture in their mind as to the opioid toxicity crisis, who is experiencing loss of life,” Dr. Gomes told The Canadian Press, adding that in some cases there may be a link between people’s overdose use and their working conditions.
This piece was also published in the Toronto Star.
Rates of opioid toxicity deaths highest among construction and trades workers, study finds

- ODPRN analysis of trends in opioid toxicity deaths among Ontario workers finds impacts across sectors, with some particularly hard hit
- Between 2018 and 2024, those who worked in construction and trades made up approximately one third of deaths from opioid toxicity in Ontario where occupation was known
- People who worked in manufacturing, hospitality and retail each made up close to 10 per cent of these deaths.
Between 2018 and 2024, those who worked in construction and trades made up approximately one third of deaths from opioid toxicity in Ontario where occupation was known, according to a report released this week by the Ontario Drug Policy Research Network (ODPRN). In addition to highlighting the toll of opioid toxicities in this sector, the report also draws attention to the impact of opioid toxicities among people across various occupations.
“People across every walk of life and every kind of job are affected by opioid toxicity, though the circumstances behind those deaths and how we might prevent them are nuanced and often differ from one workplace to the next,” says Shaleesa Ledlie, senior research associate at the ODPRN, a research group based out of St. Michael’s Hospital and Unity Health Toronto and lead author of the study. “It’s helpful for us to understand who is most affected and how, so we can tailor approaches and services to the specific needs of different people and workplaces.”
Read more about this in the Canadian Press
The ODPRN team used population-based health care data from ICES, a non-profit research institute that uses health data to produce knowledge on a broad range of health care issues. They used this data to examine the trends and circumstances surrounding opioid toxicity deaths among different employment sectors in Ontario from January 1, 2018, to December 31, 2024.
During this period, there were nearly 16,000 deaths in Ontario from opioid toxicity; approximately 3,500 of these people had an occupation included in the coroner’s report and were included in the study. The study showed that different employment sectors were affected differently by opioid toxicities, with varying rates of toxicities, trends over time and circumstances of death.
The construction and trades sector was particularly affected, with not only the highest rates of death, but also increasing rates of death over the study period.
“Our findings show that opioid-related deaths are not affecting all workers equally. Specifically, people working in industries such as construction, trades and mining experienced the highest rates of opioid-related deaths, with these deaths increasing considerably during the COVID-19 pandemic and remaining elevated over time,” says Tara Gomes, senior author of the report, a scientist at MAP Centre for Urban Health Solutions at St. Michael’s Hospital and ICES, a principal Investigator of the ODPRN, and a Professor (status) at the Leslie Dan Faculty of Pharmacy at the University of Toronto. “The reasons for this are likely multifaceted, including these occupations being male-dominated fields where people are at risk of injuries, undertreated pain, difficulty accessing treatment and barriers to discussing substance use.”
Andrzej Celinski is a co-author on the study and co-founder of the Reclaim Collective, an organization of people with lived experience that provides education and consulting services related to issues such as substance use, harm reduction, and housing insecurity.
Celinski has previously worked in the construction industry and is currently a board member for the Workers for Ethical Substance Use Policy. He says, based on his lived experience, the high rates of toxicities among workers in construction and trades was not surprising, and that workplaces could take on a greater role in harm reduction.
“Drug use in the workplace, specifically construction and trades, doesn’t get addressed very well. It’s a workplace shaped by physically demanding work, injuries and chronic pain, and a culture where asking for help can feel risky. The workplace needs to feel safe enough for people to ask for support before things become too difficult to manage on their own and they feel they have nowhere else to turn,” he says. “Making naloxone, overdose training or awareness, and connections to care more prominent in the workplace would help to reach people who might not access other traditional services, but this isn’t happening in most cases.”
Analysis points to need for tailored programs and services that address underlying factors
Other occupational sectors were also significantly affected by opioid toxicities. People who worked in manufacturing, hospitality and retail each made up close to 10 per cent of deaths.
Rates of death among people who worked in civic and government services (e.g., police, military personnel and firefighters) increased over the study period, while rates for manufacturing and transportation, warehousing and equipment operations were consistently high. The researchers note that these roles are often physically demanding, with high rates of workplace injury, chronic pain, mental health challenges and lack of support to manage transition from pain medications – all of which may increase risk.
Conversely, rates for other sectors – notably hospitality – peaked during the first years of the COVID-19 pandemic and have since decreased.
Approximately one third of people who died were unemployed at the time of death, although the hospitality sector had a higher proportion of unemployment at time of death. The researchers say that this may reflect the impact of temporary layoffs, particularly in the hospitality sector during the pandemic; it may also suggest that loss of employment, and transitions from the workforce because of injury, pain or mental health challenges may increase people’s risk of substance-related harm.
While most deaths were determined to be accidental, three sectors – civic and government services, healthcare, and administrative, financial and support services – had higher proportions of deaths by suicide.
“Taken together, these findings reinforce the need for programs and services that are tailored to the diverse needs of people at risk of opioid-related harm,” says Gomes “While workplace-based prevention, education and support remain important, with most opioid-related deaths occurring in people’s homes, efforts must also extend beyond the workplace and include reducing stigma surrounding substance use and improving access to treatment and harm reduction services to better support people across the settings in which they live and work.”
For example, underlying structural factors such as housing instability, income insecurity, and insufficient access to pain management and mental health care can all increase the risk of substance-related harm. As a result, many different harm reduction and treatment approaches are needed to keep people safe and address the underlying pain, trauma or mental challenges people experience.
“Toxicity deaths are not happening in a vacuum or to a specific group of people. Not all overdoses are happening among folks who are unhoused or in public where people can see. Oftentimes, this is happening behind closed doors and in people’s houses, often when they are alone, so it’s invisible to the population,” says Celinski.
“We need to look beyond individual behavior and address the conditions that shape folks’ ability to access support.”
Adapted from an article by Eileen Hoftyzer, writer at the Leslie Dan Faculty of Pharmacy at University of Toronto
Photos courtesy of University of Toronto, Leslie Dan Faculty of Pharmacy
Access to oral swab HIV self-testing kits expanded as part of national program

MAP scientist Dr. Sean Rourke spoke with The Globe and Mail about the launch of I’m Ready 2.0, a redesigned national program bringing free HIV self-testing and connections to care closer to people across Canada.
People across the country will now be able to order tests free of charge through the confidential program. Users of I’m Ready will also now be able to connect directly to licensed clinicians at Freddie and at Felix, two virtual sexual health services that provide HIV prevention and care.
“If we just expect people to walk in the door and get tested, there’s a certain percentage of people in Canada that will never do that, so this is an option that will actually reach them,” said Dr. Rourke.
REACH Nexus at St. Michael’s Hospital launches revamped I’m Ready 2.0, expanding free HIV self-testing access in Canada

By Andrew Russell
Toronto, ON — In a significant step toward expanding equitable access to HIV care in Canada, REACH Nexus at St. Michael’s Hospital MAP Centre for Urban Health Solutions has launched I’m Ready 2.0, a redesigned national program bringing free HIV self-testing and care connections directly to people wherever they are.
Available through a newly updated mobile app and website, I’m Ready 2.0 provides a simple, confidential, and user-friendly way for people to take control of their sexual health — no matter where they live. The platform is designed to reduce barriers to HIV testing by combining convenience, privacy, and direct access to trusted health resources.
The upgraded platform features a refreshed interface with improved navigation, making it easier for users to learn about HIV, order self-test kits, and connect with support services.
“Early diagnosis is essential to improving health outcomes and reducing HIV transmission, but too many people in Canada still face barriers to testing,” said Dr. Sean B. Rourke, Director of REACH Nexus at the MAP Centre for Urban Health Solutions at St. Michael’s Hospital. “I’m Ready2.0 centres people in care by making HIV self-testing and sexual health services more accessible, convenient, and empowering—ensuring access to the right tools and support, wherever and whenever they’re needed.”
Canadians can now access two testing options directly through the platform: the OraQuick™ HIV Self-Test, Canada’s first oral swab HIVself-test, and the INSTI® HIV Self-Test.
The addition of multiple testing options is intended to better reflect diverse user preferences and needs, and to further democratize self-testing in Canada.
“I’m Ready 2.0 reflects the strength of Ancestral Science by bringing HIV testing, prevention, and care closer to the people. When services are culturally safe and community-led, Indigenous Peoples can access care with dignity, trust, and connection to the knowledge that has sustained our Nations for generations,” said Okimâw Margaret Kîsikâw Piyêsîs, CEO, CAAN Communities, Alliances & Networks.
“The launch of I’m Ready 2.0 is about more than expanding access to HIV self-testing—it is about bringing dignity, choice, and care directly to the people who have too often been left behind,” said Nonty Nkala, a research and outreach co-ordinator at Women’s Health in Women’s Hands Community Health Centre. “We know that HIV does not exist in isolation; it is shaped by systemic inequities and the social determinants of health that continue to disproportionately impact our communities.
“By meeting people where they are with free HIV self-testing kits and seamless connections to care, we are removing barriers, building trust, and empowering individuals to take control of their health on their own terms. This is what health equity in action looks like—community-led, person-centered, and committed to ensuring that everyone can know their status and access the care they deserve.”
Beyond testing, I’m Ready strengthens pathways to care by connecting users to reliable, evidence-based information on HIV prevention and treatment. The platform also connects users directly to licensed clinicians through Freddie and Felix, making it easier to access confidential, evidence-based care for HIV prevention and ongoing sexual health support.
“PrEP is one of the most effective ways to prevent HIV, yet far too many Canadians still struggle to access it,” said Dr. Caley Shukalek, Freddie’s Chief Medical Officer.
“We’re excited to be part of I’m Ready which is helping to reimagine how people connect to HIV testing and now HIV prevention—making access faster, simpler, and more equitable so more people can get the care they need without unnecessary delays.”
Through Freddie and Felix, users can get real-time guidance on starting and staying on PrEP, understanding HIV treatment options, and accessing ongoing sexual health care—helping bridge the gap between self-testing and timely clinical support.
“Knowing your HIV status is one of the most important first steps someone can take for their health,” said Dr. Kelly Anderson, Chief Medical Officer at Felix. “What comes next matters just as much. For years, Felix has helped Canadians access licensed clinicians for PrEP and ongoing sexual health care. I’m Ready 2.0 helps connect people from testing to timely clinical care, making it easier to get the support that’s right for them.”
Since its initial launch in 2021, the I’m Ready program has reached more than 17,000 people across Canada. Between June 2021 and June2026, thousands of users have engaged with the service, including individuals testing for the first time, people living in rural and remote regions, and those who have historically faced barriers or felt disconnected from traditional healthcare systems.
Reaching people living with undiagnosed HIV has been a cornerstone of the program. Through expanded access to testing, hundreds of people have learned their HIV status and been connected to care and support. Early diagnosis opens the door to life-saving treatment, empowering people to live long, healthy, and fulfilling lives.
I’m Ready gratefully acknowledges the Canadian Institutes of Health Research and the Public Health Agency of Canada for funding this program. We also thank the Canadian Foundation for AIDS Research for its generous support and continued partnership in expanding access to HIV self-testing, helping more people learn their status, and connecting those living with HIV to care and treatment.
To learn more, go to https://www.readytoknow.ca/ or download the I’m Ready, Test app. in the Apple or Google Play stores.
About REACH Nexus at MAP Centre for Urban Health Solutions
REACH Nexus is a national research group focused on addressing HIV, Hepatitis C, and other sexually transmitted and blood-borne infections (STBBIs) in Canada. Based at the MAP Centre for Urban Health Solutions at St. Michael’s Hospital in Toronto, REACH works to reach the undiagnosed, expand testing options, connect people to care, improve access to prevention (PrEP and PEP),and reduce stigma. Learn more at www.reachnexus.ca
Media contact
Andrew Russell
Senior Communications Specialist
REACH Nexus – MAP Centre for Urban Health Solutions
andrew.russell@unityhealth.to
416-268-7642
In Memoriam: Fred Ellerington

It is with profound sadness that we share the passing of our friend and colleague Fred Ellerington, Homeless Outreach Counsellor at St. Michael’s Hospital.
With his big smile, Medicine sweater and treasured Harley Davidson, Fred was a familiar and beloved presence in the hospital and across the city. He was a tireless advocate for people experiencing homelessness, acting daily on his commitment to providing every patient with dignity and respect. Through his work, he helped bridge gaps in care, built trusting relationships and connected patients with the supports they needed to move forward. Fred was the first Homeless Outreach Counsellor for the Navigator program and was very proud to be a part of the team. He worked to establish the role and program first at St. Michael’s, and helped it grow across Unity Health and to other hospitals in Vancouver, Montreal and New Brunswick. He was excited that it will soon be launching in his hometown of London, ON.
Known throughout Unity Health and the broader community, Fred was admired not only for his expertise, but for his warmth, charisma and genuine kindness. He had a remarkable ability to make people feel seen and valued, whether they were patients, colleagues or community partners. His presence brought people together and his passion inspired those fortunate enough to work alongside him.
Fred’s warmth, generosity and dedication will be deeply missed. We are grateful for the legacy of compassion he leaves behind and extend our heartfelt condolences to his family, friends, colleagues, clients and all who had the privilege of knowing him.
A service is being planned by Fred’s family and friends. More details will be provided as they are available.
Overdose calls to paramedics on the rise in several Ontario cities, CBC analysis shows

Research by Dr. Tara Gomes is referenced in this CBC article highlighting that non-fatal opioid overdose paramedic calls surged across four Ontario cities in early 2026, nearly tripling in Hamilton and more than doubling in Toronto compared to the same period last year.
Researchers and frontline workers attribute this sharp rise to an increasingly toxic drug supply mixed with the widespread closure of public supervised consumption sites across the province.
Dr. Archna Gupta awarded CIHR Catalyst Grant to improve early pregnancy loss care

By Dr. Archna Gupta, scientist with MAP’s Upstream Lab
Why better miscarriage care matters — and what we’re building to help
As a family physician, family medicine obstetrics provider, and researcher, I care for people through many important stages of pregnancy, birth, and the postpartum period. That work is deeply meaningful to me. But over the years, I have also seen a serious gap in care for people who experience miscarriage — a common event that is still too often met with confusion, long waits, and too little support.
Early pregnancy loss, also known as miscarriage, affects up to one in four pregnancies in Canada, most often in the first trimester. Yet many individuals and families still struggle to get timely information, appropriate follow-up, and compassionate care when they need it most. In many cases, people turn to emergency departments for help, even though those settings are not designed to provide the kind of specialized, continuous support that miscarriage care often requires. The result can be repeated visits, unclear next steps, and missed opportunities to support both physical and emotional well-being.
That is why I am so excited to share that my team and I have received a Canadian Institutes of Health Research (CIHR) Catalyst Grant, “Transforming Early Pregnancy Loss Care: Co-Designing Patient-Centred Solutions”, to help improve care for people experiencing early pregnancy loss. The grant supports work that brings together patients, health-care providers, and community partners to rethink how care is delivered and how support can be made easier to access.
Our project will explore what people go through when they seek care after a miscarriage, where the biggest barriers exist, and what a better system could look like. We will work with people with lived experience, healthcare providers, and health system leaders to map patient journeys, identify gaps in current services, and learn from promising care models in Canada and beyond. We will also co-create a digital information platform, connected with the Pregnancy and Infant Loss (PAIL) Network, so people can more easily find clear guidance on what is happening, when to seek medical care, and where to turn for support.
At the heart of this work is a simple goal: no one should have to face early pregnancy loss feeling alone, unsupported, or unsure where to go. By building care with patients and communities — not just for them — we hope to create practical tools and services that are more compassionate, more accessible, and better able to meet people’s real needs across Ontario and across Canada.
Dr. Nav Persaud named Director of MAP Centre for Urban Health Solutions

Dr. Nav Persaud has been named the new Director of St. Michael’s Hospital’s MAP Centre for Urban Health Solutions, effective July 1. A highly respected scientist, family physician and champion for justice, Dr. Persaud has dedicated his career to ensuring that everyone in Canada can afford the food and medicines that they need.
“Dr. Persaud is a brilliant, creative and principled researcher who has made extraordinary contributions to the field in Canada and internationally,” said Dr. Ori Rotstein, Vice President of Research and Innovation, St. Michael’s Hospital. “I have great confidence in his leadership and look forward to seeing MAP continue to thrive under his direction.”
Under Dr. Persaud’s leadership, MAP will continue to expand its national, solutions-focused research programs to address some of Canada’s toughest public health challenges including homelessness, inequitable access to healthcare and the prevention of opioid-related harms. MAP is Canada’s largest research centre focused on health equity and the social determinants of health.
“I am deeply grateful and honoured to have this opportunity to support MAP staff and scientists as Director,” said Dr. Persaud. “Together we can build on MAP’s extraordinary legacy while striving for even greater national and global impact. We’ll work responsibly with our partners to upend the status quo by challenging systems and structures that deny people the basics needed to be healthy. Where stigma and discrimination imperil, MAP champions compassionate care and upholds the fundamental right to health for all.”
As Canada Research Chair in Health Justice, Dr. Persaud led the first-ever trial providing people with free access to essential medicines – quantifying the links between medication cost and health outcomes, and bringing to light the unfair choices that millions of Canadians are forced to make about their health. Dr. Persaud’s research directly advanced the pharmacare debate in Canada and ultimately shaped the legislation that introduced a first phase of national pharmacare in 2024. In 2025, Nav was named Chair of the Government of Canada’s National Pharmacare Committee of Experts to make recommendations on how to launch and pay for a fully single-payer pharmacare program across the country.
Dr. Persaud has been a scientist with MAP Centre for Urban Health Solutions for more than a decade. He is also a staff physician in the Department of Family and Community Medicine at St. Michael’s Hospital and a professor in the University of Toronto’s Department of Family and Community Medicine.
Thank you Dr. Stephen Hwang
St. Michael’s Hospital and MAP wish to recognize the enormous contributions of Dr. Stephen Hwang. A world-renowned scientist and Tier 1 Canada Research Chair in Homelessness, Housing and Health, Dr. Hwang became MAP Director in 2015 and has now served the maximum of two five-year terms.
Under his leadership, MAP has more than doubled in size and quintupled in multi-year funding. Despite pandemic-era research shutdowns and a major, unexpected change to the centre’s funding model, the centre has transformed from a largely Ontario-focused academic hub to a global leader in developing, implementing and scaling evidence-driven health equity solutions, with impacts that span from local to national and beyond.
Dr. Hwang’s homelessness, housing and health research program will continue to be based at MAP with a great deal of exciting work ahead, including the implementation of the Slaight Family Housing Lab, recently launched by MAP and St. Michael’s Hospital in partnership with United Way Greater Toronto. The initiative, made possible by a transformative $25 million gift from Gary Slaight and The Slaight Family Foundation, will focus on developing a new, scalable, evidence-based system to move 300 people from streets and encampments into supportive housing.
Read a Q&A with Stephen as he reflects on his eventful and impactful decade as MAP Director.
Get to know Dr. Nav Persaud
Watch: Dr. Nav Persaud testifies at the US Senate on the value of making essential medicines free for everyone (2021)
Listen: Evictions and Access to Justice with Douglas Kwan & Nav Persaud (2022)
Toronto Star:
- Opinion: Here’s one thing Mark Carney could do that would improve the welfare of more Canadians than any pipeline or mine (2025)
- He never learned about Canada’s first Black doctors in medical school. He wants all students to know their names (2023)
- He’s been called a ‘lethal force’ who’s not afraid to take on medical authorities. And it all started with pain week (2018)
Thank you Dr. Stephen Hwang: Celebrating more than a decade of MAP leadership
On June 30, 2026, Dr. Stephen Hwang will conclude his tenure as director of St. Michael’s Hospital’s MAP Centre for Urban Health Solutions, Canada’s largest research centre focused on health equity and the social determinants of health.
A world-renowned scientist and Tier 1 Canada Research Chair in Homelessness, Housing and Health, Dr. Hwang took on this role in 2015 and has now served the maximum of two five-year terms – plus one “bonus year,” as he jokingly calls it (his first term was extended due to the pandemic).
Although Dr. Hwang is leaving big shoes to fill as director, he isn’t going far. His research program will continue to be based at MAP under his leadership with a great deal of exciting work ahead.
Transformative, national impact
Dr. Hwang’s legacy as MAP director is nothing short of extraordinary. Under his leadership, MAP has more than doubled in size and quintupled in multi-year funding.
Despite pandemic-era research shutdowns and a major, unexpected change to the centre’s funding model, the centre has transformed from a largely Ontario-focused academic hub to a global leader in developing, implementing and scaling evidence-driven health equity solutions, with impacts that span from local to national and beyond.
Through it all, Dr. Hwang’s approach has been grounded in his commitment to “servant leadership,” supportive team building and above all, a deep respect for his partners’ and colleagues’ unique perspectives and experiences.
We talked with Stephen to reflect on his eventful and impactful decade in the role.
Q: Looking back over the past 11 years, what are some highlights that you’re most proud of?
When I started in the role, MAP had just lost our core provincial funding. We had to quickly pivot to a philanthropic model, but it wasn’t clear how to do that. Working with the St. Michael’s Foundation and their incredible volunteers to get that first fundraising campaign off the ground, and realizing that there was indeed donor interest with the potential to sustain MAP, was a big moment. It felt like a huge turning point for the organization.
Our Solutions for Healthy Cities symposia were also major highlights for me. They have all been so inspiring, and great to be together in person.
I’m thankful and extremely proud of our national Even the Odds partnership with Staples Canada and how it’s grown, thanks to Staples’ leadership and vision. It has pushed MAP to get even more ambitious about our geographic reach and impact, and enabled us to scale our work in ways we could only have dreamed of 10 or 11 years ago.
Finally, I wouldn’t call it a highlight, but leading the centre through the pandemic was an honour. It was an extremely difficult time, but we pulled together at MAP and pivoted very quickly to fill an urgent need for research on COVID-19 and how to improve access to care and support during lockdowns.
Q: What’s been the hardest part of the job?
My first instinct is to always be as egalitarian and non-hierarchical as possible as a leader and to practice servant leadership. However as director, I also had to learn that sometimes a leader must make tough decisions based on their own best judgment. There are some decisions you can’t take a vote on, and also some decisions that not everyone will agree with. In those situations, I reflected on MAP’s and my own values and principles, I thought very carefully about appropriate and fair processes, and I sought the advice of wise counsel. Those things were all very helpful, but it was still something I had to learn to do.
Also, back to the pandemic – that was definitely hard. Our people at MAP were dealing with so much. For me, oddly, between leading MAP and working as a general internist at the hospital, the most straightforward part of the pandemic was my work taking care of patients with COVID. That part was squarely within my professional experience. At MAP, I had to figure out how to support our people who were struggling in all sorts of different ways, because of other stresses that the pandemic was causing. That part was much more complex.
Overall though, I have to say, it’s been a really wonderful 11 years. Some of our challenges have moved us forward to a better place. For example, looking back, I really believe that the transition to philanthropic funding made our research better. Many of our donors are leaders in the private sector. They ask us tough questions and challenge us in important and ultimately very positive ways. We were always impact-focused at MAP, but through our dialogue with donors we have had to get crystal clear on exactly how our work is helping people.
Q: What’s next for you?
My MAP research program has just launched a major partnership with United Way and the City of Toronto called the Slaight Family Housing Lab. Together, we were extremely fortunate to receive a $25 million gift from Gary Slaight and the Slaight Family Foundation to fund the development of a new, scalable, evidence-based system to move people from streets and encampments into supportive housing. I’m really excited about the potential impact. It’s going to be a huge focus for me in the coming years, and I believe it will lay the groundwork for similar work across the country.
Leading MAP has been a tremendous honour. I’m so happy to continue to be a part of it.